Mild bleeding may happen during the first trimester in about 20% of pregnancies. It usually passes smoothly, but consulting your doctor is of utmost importance to reach a diagnosis of the cause of bleeding, identify the degree of risk and plan a suitable treatment.
On the other hand, bleeding beyond the first trimester (13 weeks), especially after 20 weeks, is more dangerous and you should consult your doctor as soon as possible if you get any bleeding then.
What are the causes of bleeding in early pregnancy?
During the first half of pregnancy, bleeding is usually due to threatened miscarriage. This is mild bleeding and/or blood collection inside the womb (next to the pregnancy sac). It usually ends safely with no effects on the growth and development of your baby.
The other causes include silent miscarriage, where the baby’s development may be abnormal leading to its failure to thrive and the need to terminate the pregnancy.

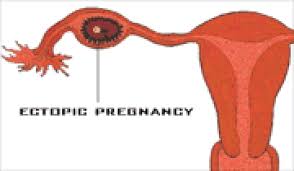
Or bleeding may be due to an ectopic pregnancy, where the pregnancy sac actually implants outside the normal uterine cavity (usually in the fallopian tube). This is an emergency condition which may lead to complications and needs early management, usually surgically.
Other rare causes include vesicular mole pregnancy, where the pregnancy tissue turns into some type of benign tumor growing within the womb instead of the baby. This condition needs evacuation of the uterine cavity then strict follow up for the following six months then in every subsequent pregnancy.

What about the causes of bleeding in late pregnancy?
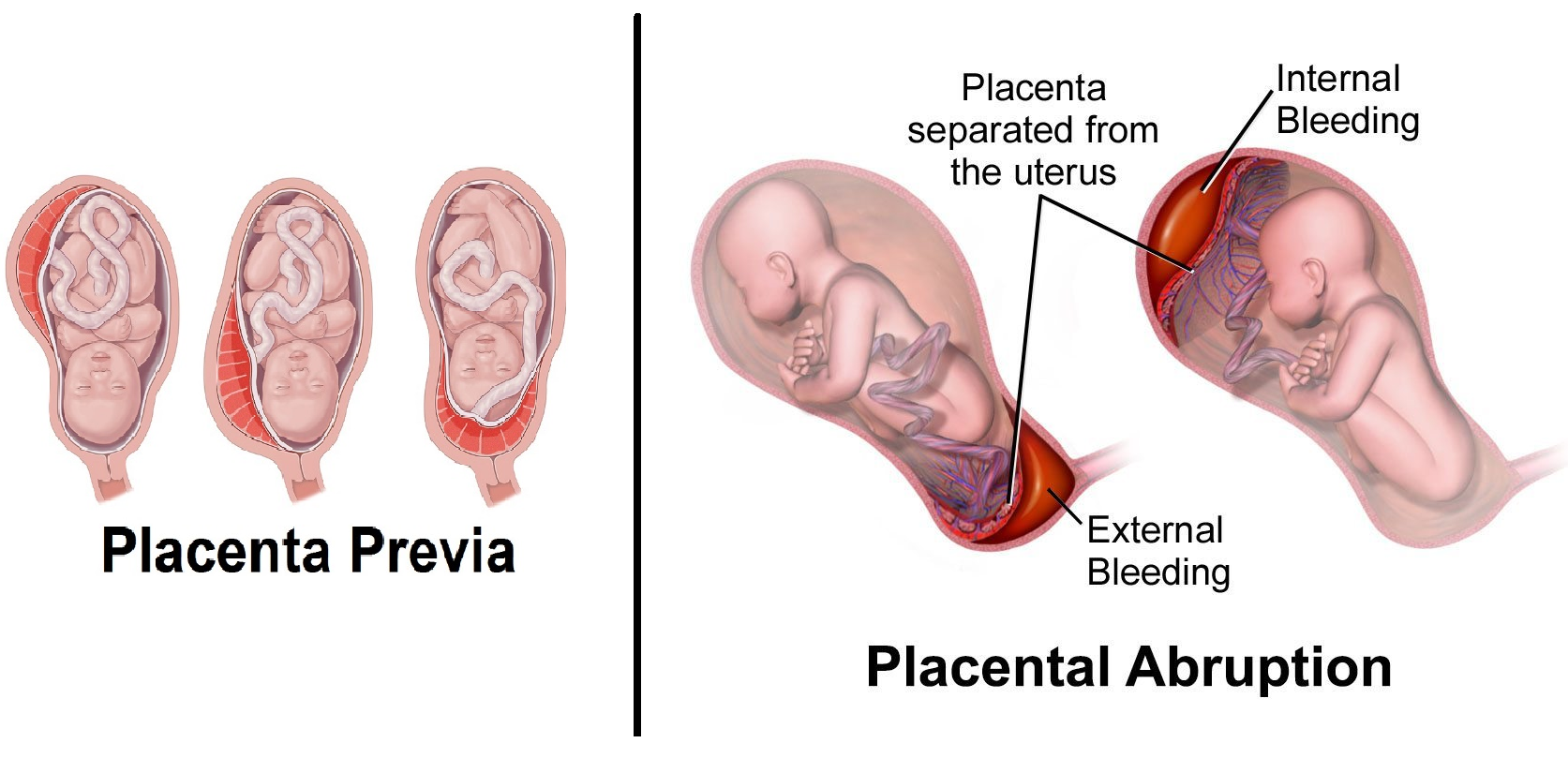
The most common cause of bleeding during the second half of pregnancy is due to placental abnormalities. Such as placental separation or abruption, which is an emergency condition that usually necessitates urgent delivery, or placental implantation in the lowermost part of the womb (uterine) cavity.
The latter usually presents with recurrent attacks of painless bleeding getting more frequent and more severe as pregnancy advances. These conditions need hospitalization in anticipation of surgical intervention should the bleeding get more severe. It is often possible to postpone delivery till the last few weeks of pregnancy if the bleeding is not severe, and the baby is developing normally.
How do you reach a diagnosis regarding the cause of bleeding?
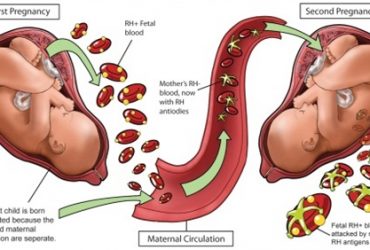
The main diagnostic tool is ultrasonographic evaluation of the pregnancy, both per abdomen or transvaginally. Both ways are safe to use and do not harm the pregnancy. Blood tests would diagnose anemia and may identify the women with Rh-negative blood group, thus needing Anti-D injection.
What should I do if I develop threatened miscarriage?
The best first treatment is resting at home as possible and follow up of fetal development by serial ultrasound scans. It may be best to avoid sexual intercourse for a while until things settle down. Some medicines may be used to reduce the risk of losing the pregnancy, such as natural progesterone hormones. This is a hormone which is normally produced during pregnancy to relax the womb muscle wall to prevent contractions. It is also important to exclude fetal abnormalities prior to deciding to help the pregnancy to carry on. Generally, most pregnancies with abnormal embryos would, sooner or later, end in complete miscarriage, while most pregnancies with normal embryos survive and end successfully.
Best Regards
Dr. Sherif Ahmed Ashoush