What is Preterm Delivery?
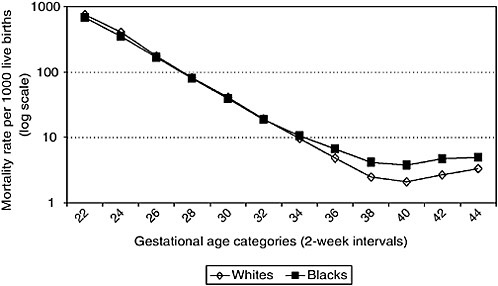
It is delivery at 28 (mid sixth month), when the baby develops any chance of survival at birth, to 37 weeks (first week of the ninth month), when the baby is mature enough to minimize any risk of post-delivery need for neonatal intensive care. Taking in consideration that Normal pregnancy is 40 weeks and that delivery prior to 28 weeks is generally considered a miscarriage since the neonatal survival rate is very low at such stages.
What are the risks of preterm delivery?
Obviously, the rate of complications drops the closer delivery is to 37 weeks.
The main risk concerns the baby’s health condition, since a premature neonate (<37 weeks old) is not ready yet for survival after birth with poor respiration, suckling and immunity. In premature babies, the body’s ability to maintain an adequate temperature or to stop bleeding following minor trauma are still defective. Hence, the vast majority of premature babies need to be admitted to a Neonatal Intensive Care Unit (NICU) under continuous medical follow up. Furthermore, these babies are more liable to long-term chronic diseases such as respiratory/chest conditions, hearing and vision defects, low intelligence coefficient, and neurological diseases.
What are the causes of premature delivery?
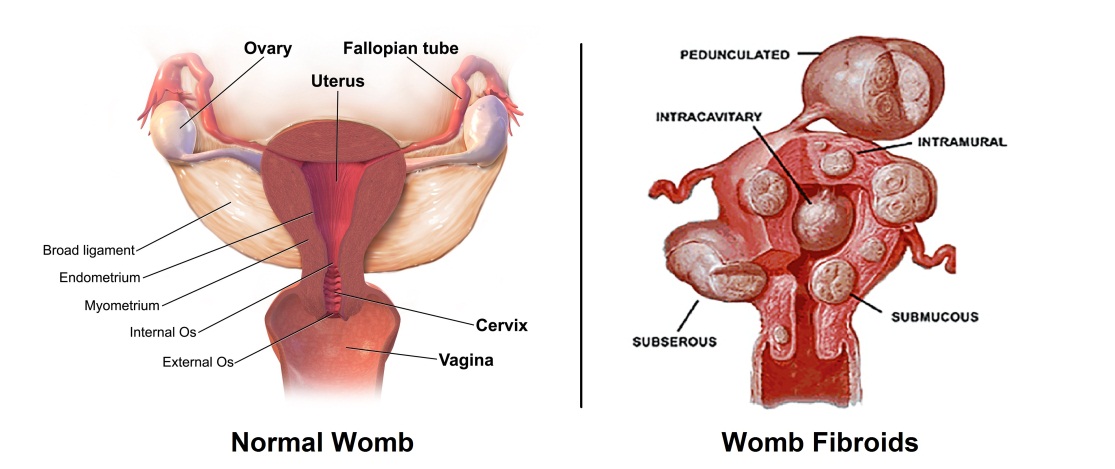
Some cases are due to weakness of the cervix (neck of the womb). Some are due to a to small womb (uterine) cavity whether due to intrauterine adhesions, benign lumps (e.g. fibroids) or congenitally small uterine cavity.
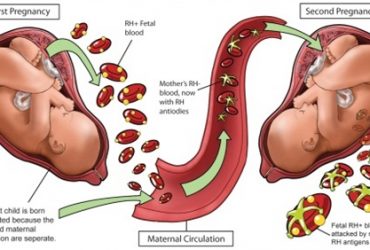
 Some other cases are due to chronic infections in the neck of the womb leading to irritability of the womb muscles or premature rupture of the membranes (breaking of the waters) necessary for fetal survival inside the womb. Other causes of premature delivery include several diseases causing poor blood flow in the uterine and umbilical arteries. Some immune defects may increase the risk of prematurity by immune attacking of the placenta and the baby. This last cause usually leads to earlier miscarriage rather than premature delivery. The cause of prematurity may also be related to maternal general health, such as hypertension, twin pregnancy, smoking or poor nutrition.
Some other cases are due to chronic infections in the neck of the womb leading to irritability of the womb muscles or premature rupture of the membranes (breaking of the waters) necessary for fetal survival inside the womb. Other causes of premature delivery include several diseases causing poor blood flow in the uterine and umbilical arteries. Some immune defects may increase the risk of prematurity by immune attacking of the placenta and the baby. This last cause usually leads to earlier miscarriage rather than premature delivery. The cause of prematurity may also be related to maternal general health, such as hypertension, twin pregnancy, smoking or poor nutrition.
How can we prevent premature delivery?
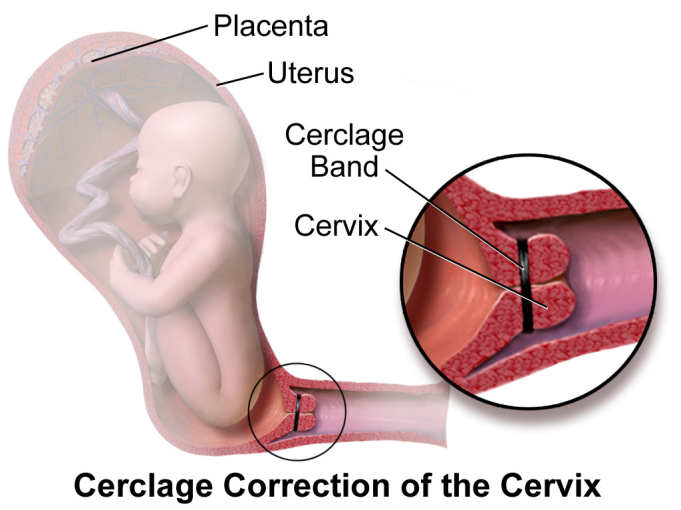
There is no one-for-all treatment which would be successful in all cases. It rather depends on the cause in any specific lady. Weakness of the cervix, for example, is best treated by progesterone medication +/- cervical cerclage (placing a stitch to hold the neck of the womb). The latter is usually done at the end of the third month through a vaginal approach, but may rarely need an abdominal incision in more difficult cases.
Treating infections in the cervix is through antibiotics. Some cases, where the womb starts contracting prematurely in an attempt to expel the baby, may benefit from some types of medicines which stop uterine contractions. There are several types of such drugs, an experienced specialized doctor can decide the best type for every case.
Treatment also needs close follow-up. Some cases may need bed rest and/or hospitalization for intravenous medications. Cases of immune defects or poor blood flow may sometimes benefit from some medicines normally used for allergy or immune diseases (steroids, blood thining injections or intralipid infusions). There is also a different type of injections which help accelerate the fetal lung maturity and reduce internal bleeding following premature delivery.
How may I know if I am at risk of premature delivery?
Prematurity is more common in presence of a history of previous miscarriage or preterm delivery, or in presence of bleeding during the current pregnancy, fetal congenital malformations or growth restriction, increased amount of amniotic fluid, and maternal hypertension or diabetes mellitus.
Measuring the length of the neck of the womb through an internal scan during the first half of pregnancy may predict an adequate number of cases.

But, at the end, some cases are very difficult to predict and have no clear cause. And hence, there would always be an important role for adequate Neonatal Intensive Care Units (NICU) should preterm delivery happen.
What is the safest way of delivery for premature babies?
In a generally healthy baby with adequate presentation (head first), vaginal delivery remains the preferable way, taking into consideration that emergency cesarean section may still be needed should the baby go into any distress during labor. On the other hand, breech presentation (bottom first) is generally advised to be delivered by cesarean section.