I am pregnant and I was diagnosed as hypertensive. Does this carry any special risks for me or my baby?
The risks associated with hypertension during pregnancy can be minimized with adequate treatment and strict follow up. But this treatment depends on the type of hypertension you have.
The cause of your high blood pressure may just be a pregnancy induced hypertension in late pregnancy, which should be easy to control in pregnancy and should disappear after delivery. Or it may be due to chronic long-standing hypertension where high blood pressure will persist after delivery, although it may become less severe. Therefore the effects of long standing hypertension on pregnancy outcomes are usually mild as long as the blood pressure is kept under control by different lifestyles and medications.
On the other hand, high blood pressure due to chronic diseases in the kidneys, the thyroid or adrenal glands, or cardiovascular diseases is a more risky condition which may occasionally indicate hospitalization or even preterm delivery.
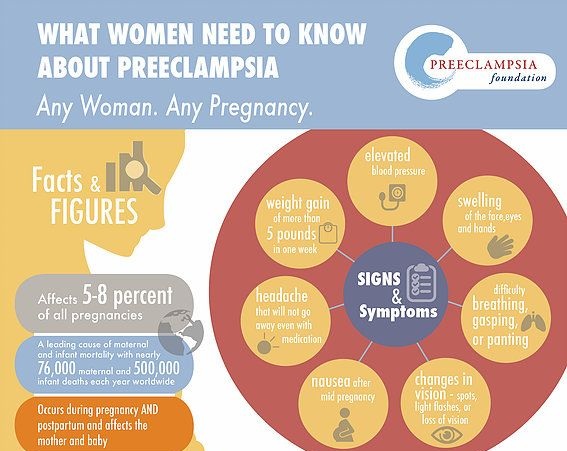
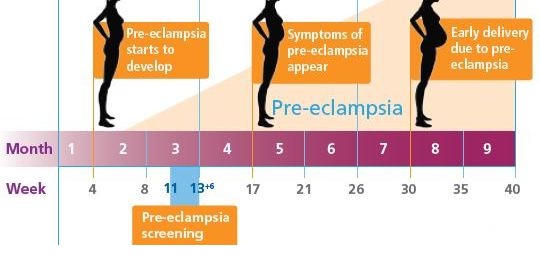
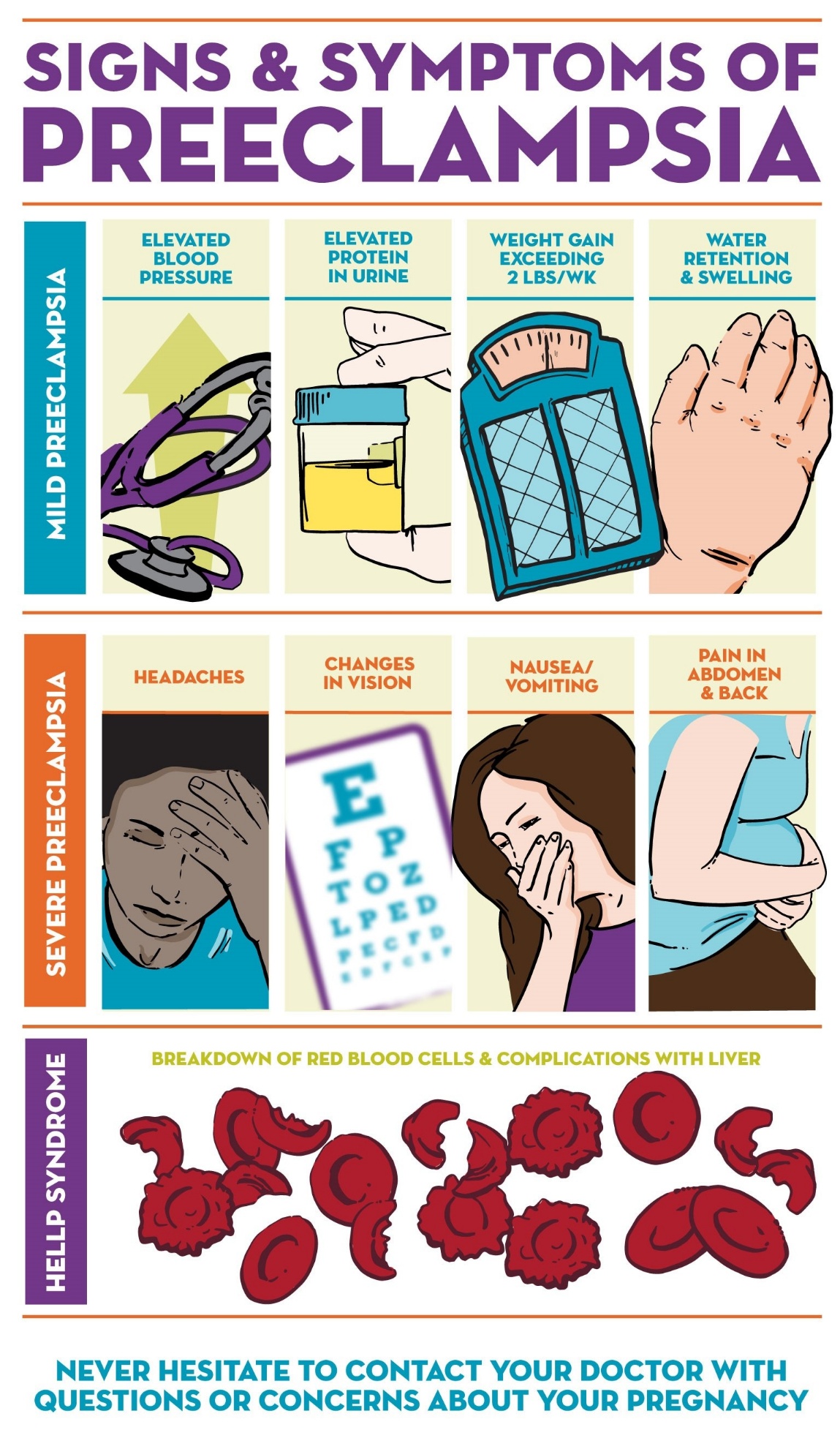
Last, but not least, is the pregnancy-induced hypertension (known as preeclampsia). This is the most serious type of hypertension in pregnancy, requiring early and swift intervention as it may otherwise lead to serious consequences.

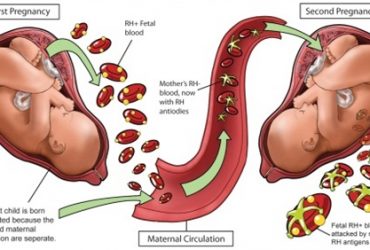
What is Preeclampsia, and what are its associated health risks?
It is elevation of the blood pressure during the second half of pregnancy for no chronic reason. It is more common in your first pregnancy, if you are pregnant wit twins, or if you suffer with diabetes mellitus, some immune diseases (such as systemic lupus erythematosis).
The only true cure for such condition is delivery. But if the lady is still in early pregnancy stages, the obstetrician may try to postpone delivery to give the newborn a better chance of survival. This is of course on the condition that the lady’s blood pressure is controlled and she has more or less normal organ functions on blood testing.
We recommend frequent monitoring of blood pressure, blood tests and fetal wellbeing till to reach a gestational age that carries fair chances of neonatal survival following birth. This is, of course, on the condition that the lady does not suffer from any complications such as severe uncontrolled hypertension, deteriorated liver or kidney functions, impaired vision, fetal distress or other risks such as placental separation (abruptio placentae), cerebrovascular strokes or convulsions.
How may I know the cause behind my hypertension?
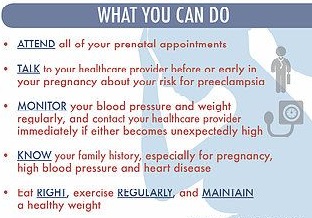
This is through clinical and laboratory evaluation by a specialized doctor. This is, actually, one of the main benefits from routine pregnancy care. Only then, you can diagnose any problem early enough to allow treatment and prevention of complications.
May I use my hypertension medications safely during pregnancy?
Not all medicines are safe to be used during pregnancy, for example ACE inhibitors such as Capoten or Capozide are contraindicated during pregnancy, diuretics are also best to be avoided if possible. On the other hand, aldomet, epliat, trandate, aprisoline and atenolol are safe to use. Most cases start on of the first three drugs, then the dose is adjusted till to reach a controlled blood pressure.
But I need to make one thing very clear, if uncontrolled hypertension is due to preeclampsia, then the true cure is by delivering the lady rather than starting a new antihypertensive medicine.
What symptoms should I report to my obstetrician during antenatalcare?
You should report any nausea, dizziness, impaired vision, vaginal bleeding or reduced fetal kicks. Please do not wait till your next antenatal care visit, but rather report these complaints as soon as possible, since they may, rarely, point to an underlying serious issue. Your doctor will order some tests to diagnose any deterioration in your condition which may occasionally indicate hospitalization or even delivery.
What if I am still far from my due date of delivery?
Here, you need a well-equipped hospital, with a blood bank, an intensive care unit, and a special care baby unit. Sometimes, you may have an induction or augmentation of labor aiming at vaginal delivery if the condition of baby and yourself allow it. But frequently, this may mean having to wait for long hours before delivery and thus a cesarean section is a common resort. It is worth explaining that you or your newborn may need admission to intensive care units to allow the best possible degree of care.
Does delivery end the risk associated with preeclampsia?
Yes, most cases start to improve within 1-2 days after delivery, and may be back to normal by the end of the first week, unless there were serious complications in the body functions requiring longer treatment. As for the other causes of chronic hypertension, the condition may slightly improve but is never cured by delivery, so these cases need following up their blood pressure regularly postnatally.
May I suffer with hypertension in my next pregnancy?
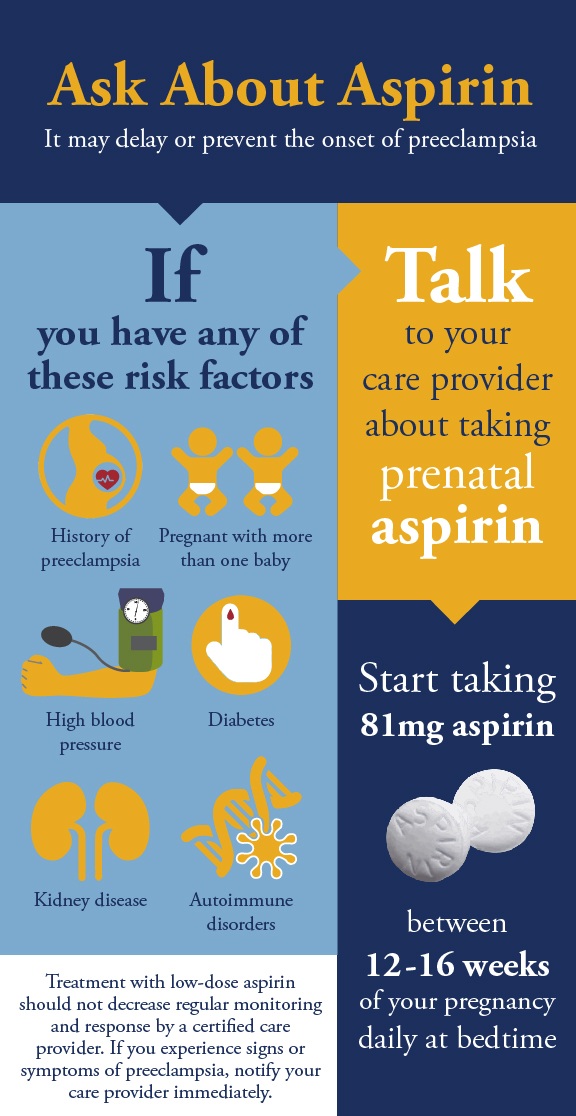
Preeclampsia is usually a disease of first pregnancies, unless you get severe early onset preeclampsia, or you suffer from an underlying risk factor such as diabetes mellitus, vascular, autoimmune or kidney disease. In such cases, using low dose aspirin, calcium and vitamin D supplements helps reduce the risk of recurrent preeclampsia in future pregnancy.
Wishing you a safe and healthy pregnancy